The years have passed mighty quick for me as I find myself now aged 53.
I’ve been super busy raising a family, as well as running my clinic and the continuing education that goes along with that.
Just recently, I have noticed my menstrual cycle has disappeared.
My goodness, I am beginning menopause – I am perimenopausal!
Other than an obvious weight gain (which I put down to the pandemic stress), I personally haven’t had many other obvious signs to suggest this.
However, this is not the norm I can tell you now. So many of my clients come to me for help in relation to so many menopausal symptoms. The most popular being excessive menstrual bleeding, hot flushes, headaches, mood swings, vaginal dryness, and low libido.
So, let’s dive in ladies and learn just what goes on in our bodies as we mature.
What Is Menopause?
Menopause is the natural stopping of a woman’s menstrual cycle, with the ovaries no longer releasing an egg every month.
Menopause is signalled by 12 months since last menstruation and it marks the end of fertility.
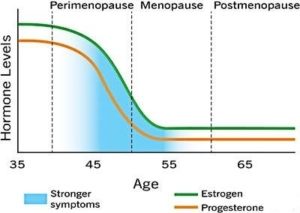
The transition period in the lead up to menopause is called perimenopause.
Most women experience full menopause by the age of 52, but pelvic or ovarian damage may cause sudden menopause earlier in life. Genetics or underlying conditions may also lead to early onset of menopause.
Many symptoms result from unevenly changing levels of our female hormones (progesterone and oestrogen), leading to a condition known as oestrogen dominance.
What Is Oestrogen Dominance?
Menopause symptoms together with a range of other ailments including osteoporosis, PMS, weight gain and cancer have all been linked to oestrogen dominance.
In a healthy woman two vital hormones, progesterone and oestrogen, are maintained in equilibrium. When progesterone levels drop in proportion to oestrogen this can lead to the effects of unopposed oestrogen taking root.
Progesterone levels drop ahead of oestrogen production leading to oestrogen dominance – a high oestrogen level compared to progesterone.
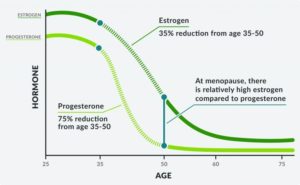
In most women, hormone levels start to decline around their mid-thirties, gradually at first, then accelerating through their forties, before levelling out between 50 and 55.
However, when this decline commences, progesterone production falls considerably faster than oestrogen. The result is a widened gap in the levels of these two hormones which does not right itself until hormone levels finally stabilize in the years following the menopause.
This natural change in hormone levels is aggravated by modern environmental and lifestyle factors, which are believed to be responsible for the increasing incidence of oestrogen dominance.
Taking small amounts of natural progesterone actually relieves many of the symptoms thought to be caused by oestrogen deficiency.
In cultures where diets still largely comprise a variety of fresh vegetables, progesterone deficiency remains rare. Plants produce substances that behave much like progesterone and as such when the body’s progesterone production winds down, these substances are able to counteract the effects of oestrogen. In western cultures, where processed foods form the bulk of diets, these nutrients are largely absent.
For women in modern societies, the problem is accentuated through increased exposure to oestrogenic substances in the form of environmental pollution and toxins as well as extended use of birth control treatments.
Read my article on XENOESTROGENS for further information.
This combination of increased oestrogenic exposure and reduced natural, progestogenic nutrients, accentuates normal changes in hormone levels creating a ‘perfect storm’ for oestrogen dominance.
That’s got you thinking I’m sure about your symptoms, right? Are your current symptoms actually linked to menopause?

Symptoms of Menopause
In menopausal women, oestrogen dominance can lead to common symptoms:
- Acceleration of the ageing process
- Allergies, including asthma, rashes, sinus congestion, and autoimmune disorders
- Breast swelling and pain
- Cervical Dysplasia
- Cold hands and feet, relating to thyroid dysfunction
- Decreased sex drive
- Depression with anxiety or agitation
- Dry eyes
- Early-onset of menstruation
- Fat gain, especially around the abdomen, hips, and thighs
- Fatigue
- Fibrocystic breasts
- Gallbladder disease
- Hair loss
- Headaches
- Hot flushes
- Hypoglycaemia
- Inability to focus
- Increase blood clotting/stroke
- Increased heart rate
- Infertility
- Irregular menstruation and bleeding
- Insomnia
- Loss of libido
- Memory loss
- Miscarriage
- Mood issues (PMS, anxiety, depression, irritability)
- Night sweats
- Osteoporosis
- Pre-menopausal bone loss
- Sleep issues
- Sluggish metabolism
- Uterine cancer
- Uterine fibroids
- Vaginal dryness
- Water retention, bloating
- Weight gain ….AND MORE
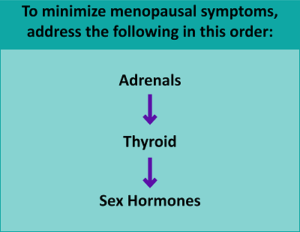
Increased Menopausal Symptoms: A Sign Of Adrenal Cortisol Imbalance
Women can have an underlying adrenal cortisol imbalance contributing to their perimenopause and menopausal symptoms.
Progesterone has distinct effects on reproduction but also influences almost all tissues in the body.
Like many hormones, progesterone is made in multiple tissues in the body. The second greatest amount in young women is made in the adrenal glands. The majority of this progesterone is used to make cortisol, but some become available to contribute to the other cells in the body.

In young women, the vast amount of progesterone available to the body comes from ovarian production as the graphic below shows.

This balance gradually shifts towards a general decline in ovarian production but the contribution from the adrenal glands should be maintained. With this combination, the adrenal glands become the dominant source of progesterone as menopause progresses.

Healthy progesterone balance going into perimenopause is dependent on healthy adrenal gland function.
Stressed adrenal glands result in greater symptoms during this transition. Those who are having lots of symptoms during this transition should consider having their adrenal function assessed.
Assessing thyroid function thereafter is vital since hypothyroidism (an under-active thyroid) and menopause have many overlapping symptoms. Having both conditions may increase the risk and severity of these symptoms.
Thyroid disorders may also increase your risk for long-term complications of menopause, such as osteoporosis and cardiovascular diseases.
Need Help With Your Hormones?
Balancing hormones is complicated and best done with a qualified practitioner.
If you wish my assistance, simply BOOK A CONSULT with me today.
*If you’ve got this far – thank you for reading and I look forward to bringing you more information in the future.
Now, enjoy a subliminal menopause message before bed each night …